Authors:
Ellen Isaacs, MD, New York Medical College (retired) and
Karyn Pomerantz, MLS,MPH, George Washington University (retired)
Reviewers:
People’s CDC Standards Review Team Member who cannot be named
Rita Valenti, RN
Josh Garoon, PhD, University of Wisconsin-Madison
Elaine A. Hills, PhD, Independent Public Health Scientist
From the point of view of public health, there are two overwhelming reasons to promote global vaccination against COVID-19:
- Since 2020, there have existed vaccines which are highly effective at preventing death and serious illness. Thus, it is incumbent on all of us concerned with prioritizing human health to demand that all people of the world have access to, and education about, these vaccines.
- When we allow large population groups to remain unvaccinated, the virus will have ongoing opportunities to mutate, creating variants that may be more lethal than the original virus strain or earlier variants and/or vaccine-resistant. This endangers the health of the whole world, including those already vaccinated.
THE STATUS OF THE DISEASE and VACCINATIONS

By early April 2022, the World Health Organization (WHO) reported over 500 million cases of COVID-19 that had resulted in 6.1 million deaths globally,[1] but a worldwide estimate based on excess mortality puts the likely figure at 18.2 million, which includes many deaths in low income countries.[2]According to the New York Times World Vaccination Tracker on April 4, 2022, 66.2%% of the world population has received at least one dose of vaccine, but only 15% of people in low income countries have had at least one dose. In Burundi the total percentage considered fully vaccinated (who received the full primary series but without a booster) is 0.1, in Congo 0.5, Chad 0.9, and Haiti 1.0. Altogether, 15 African countries have a vaccination rate under 10%. A few countries, such as the United Arab Emirates, Portugal, Brunei, Chile, Malta, and Cuba are at 94% or above; China is 91% and the US is 65% fully vaccinated.[3]

About 57% of the world has received their primary series (without booster), which has required approximately 10,935,000,000 doses of various vaccines.[4]It would require about 8.25 billion doses to provide individuals throughout the world their primary series, and then another 7 billion or so doses to boost everyone once, depending on the eligibility of children. The WHO estimates that the pandemic would end this year if 70% vaccination is achieved, which is very unlikely to occur, and many now think vaccine resistant variants could alter this calculation.[5]
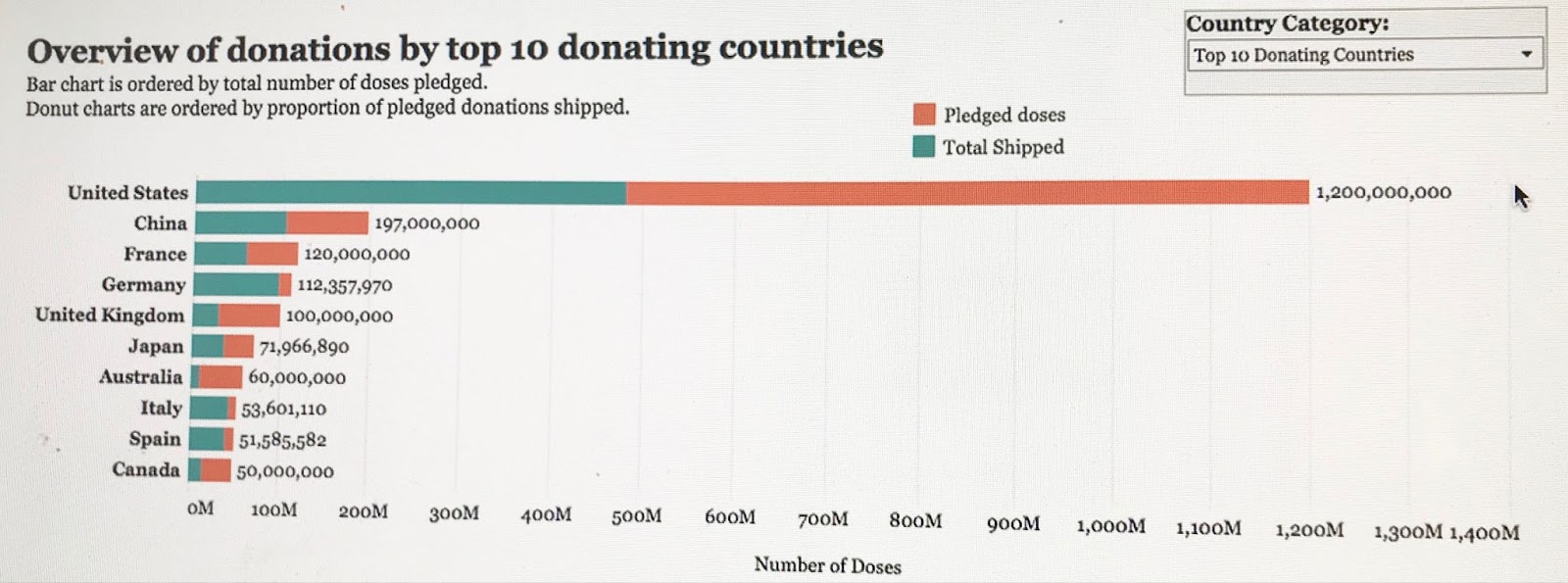
According to an analysis published in STAT news, the G7 and EU nations will have 1.39 billion excess mRNA doses as of the end of March, 2022, assuming that 80% of all adults are vaccinated and boosted, but there is a plan to give only 500 million away.[6]The US has donated more than 524 million doses worldwide as of April 15, 2022 and has promised 1.2 billion more.[7]It is estimated that it would cost $12.5 billion to produce the required promised doses. On April 5, the Senate declined to spend $5 billion to finance international vaccines.[8]
THE DANGER OF LOW VACCINATION RATES
That so many millions remain unvaccinated virtually assures that new viral variants[9] will emerge. As the COVID 19 virus – mRNA genetic code strands enclosed in a lipid sphere with protein spikes – enters host cells, it is copied and reproduced and travels into new cells. There are frequent copying mistakes in this process, like those made when redrawing a picture over and over, resulting in an altered virus. Most of these changes are of little consequence as they make the virus less potent or do not change the ability of the immune system to react. But some changes will make the virus more dangerous – more infectious, causing worse disease, or less recognizable by antibodies. Variants are more likely to arise the more bodies the virus has to infect and the longer it lives in each one, both of which are determined by immunization status and underlying health of the patient. Thus, as long as nearly half the world remains unprotected, it is inevitable that new variants will keep coming and some may be very bad for us.[10]This is what happened when the original strain mutated into the later Delta and Omicron variants.
BUT WHERE ARE THE VACCINES?
Currently there are eleven vaccines that are being used around the world, including three made in China, three in India and Russia, Astra-Zeneca in the UK, and Johnson & Johnson (production paused) and Novavax (pending US approval) in the US in addition to the two mRNA vaccines developed by Pfizer/BioN Tech and Moderna. According to a recent literature review published in January 2022 in the International Journal of Infectious Disease, all the vaccines had effectiveness in phase 3 trials ranging from 59%-98%.[11] Of course, the passage of time and emergence of new variants will greatly affect these results. Of all the vaccines, the mRNA have been noted for being highly effective at preventing hospitalizations and deaths, resulting in as much as a 20-fold reduced risk of death after boosting.[12] However, recent evidence shows that the Johnson & Johnson vaccine may provide more long-lasting protection than mRNA vaccines against both transmission and hospitalization,[13] despite concerns about the Johnson & Johnson vaccine’s side effects.[14]
mRNA vaccines are also the most efficient to manufacture because they do not require biologic cells to produce and are the simplest to reprogram for new variants.[15] The process of producing a modified vaccine can take seven days as opposed to a few months for those that require cellular growth and could potentially be made by many manufacturers in Africa and several in Asia and South America.[16]
WHAT IS BEING DONE
The ability of companies in low and middle income countries to make mRNA vaccines has been limited by intellectual property laws that control who can manufacture a product. Currently, the World Trade Organization (WTO) Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) requires signatory countries to allow pharmaceutical companies to have monopoly patent protections for their medical products. It should be noted that the WTO only came into existence in 1994, and for the first time Western nations were able to enforce patents on medicines and other technologies in return for concessions to poorer nations offering wider access to rich northern markets. In truth this provision marked the end of a massive 20 year campaign by pharmaceutical companies alarmed at the manufacture of generics by India since the 1970s.[17]
Although the WHO and the US have agreed to waive TRIPS laws, the EU, Switzerland and Germany have not. A new compromise just announced allows self-declared developing countries to produce and export vaccines to other eligible countries and to lump all existing patents together. However, the waiver does not apply to diagnostics or therapeutics.[18]
Despite the fact that Moderna received $10 billion from the US government to develop its vaccine, and although they claim they will not enforce patent protections, Moderna refuses to share the knowledge and technology necessary to actually produce their COVID-19 vaccine. The US government has the authority under the Defense Procurement Act (DPA) to require Moderna to share vaccine technology with the WHO mRNA hubs but has not done so. Meanwhile, Pfizer and Moderna have made approximately $54 billion from sales of their mRNA vaccines; Pfizer’s projected profits for November 2021 were $36 billion, and Moderna’s $18 billion.
All of the COVID-19 vaccines have one thing in common: the need for cold-chain storage, ranging from around –70°C (–94°F) during specialized shipping to around 2 to 8°C (36 to 46°F) when administered, but only the mRNA vaccines require super cold storage. However, elaborate analyses have been done as to how the obstacles to transporting, storing, and administering vaccines could be overcome in low income countries with various climate and developmental obstacles.[19] What is lacking is the investment and the will. Even the newly appointed White House COVID Czar, Dr. Ashish Jha, has been an unpaid consultant for Albright Stonebridge. This strategic advisory firm advised Pfizer against suspending intellectual property laws and downplayed the ability of other countries to produce mRNA vaccines.[20]
COVAX, a multinational agreement sponsored by multiple international institutions such as WHO and UNICEF, was supposed to facilitate the delivery of vaccines to all nations. However, it has accounted for less than 5% of all vaccinations administered globally. A major factor has been the direct deals between high income countries and pharmaceutical companies. The United States has entered into seven deals with six companies for 800 million doses, which are enough to vaccinate 140% of its population.[21]COVAX then allowed self-paying nations to choose what vaccines they would receive for up to 50% of their population. Donations by individual countries are highly inadequate to meet the need, nor have their pledges been fulfilled.
A potential game changer is the development of Corbevax, a vaccine designed by Drs. Maria Elena Bottazzi and Peter Hotez at Baylor College of Medicine, which is to be produced and distributed without patents or profit, financed only by no-strings-attached private donations. It is a two-dose protein subunit vaccine, similar to that for hepatitis B, that can be stored in a regular refrigerator and will cost less than $2 a dose. It has been found to be safe and effective in phase 3 trials but, with its effectiveness so far measured only by antibody response,[22] how that translates into clinical effectiveness in preventing transmission and reducing disease severity is not yet certain. Corbevax has been licensed in India, Bangladesh, South Africa, and Botswana to date, with pending deals in Vietnam and Taiwan.The Indian manufacturer, BioE, plans to produce more than one billion doses for developing countries, so it will reach more people than what’s been shipped by the wealthiest nations.[23] [24]
CONCLUSION
Vaccination rates remain highly unequal around the globe, reflecting the priority of profits over people in our international capitalist world. The Black population of Africa, with its overall vaccination rate of 11%, is far less protected than any other area, which even outstrips the two-to-three- fold racial inequalities of sickness and death within the US. Given the hesitancy of several wealthy countries to waive patent protections, the unwillingness of manufacturers to share technology, and the failure of high income countries to donate adequate vaccine doses, the situation will not improve soon unless Cobrevax proves effective and is able to be rapidly produced and administered. Existing disparities almost guarantee that new and possibly more dangerous and/or vaccine resistant COVID-19 strains will emerge, for which the whole world will pay a price. Indeed, the greed of the pharmaceutical industry and the governments which promote them has prevented a path to the resolution of this pandemic in all countries, but the capitalist short sightedness of reckoning quarterly profits is not to be overcome, even as a matter of long range self-interest, even of life and death. Rapid and equitable action against COVID-19 depends on us, on building an international movement of ordinary people, scientists and health workers to demand that public health, not wealth, is the priority. This means not only vaccinating the world but encouraging public health measures like masks, quarantines, and social distancing, which are being prematurely discarded – another manifestation of profits over people.
REFERENCES
[1] https://covid19.who.int/table (Accessed April 15, 2022)
[2] https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)02796-3/fulltext#seccestitle10
[3] https://www.nytimes.com/interactive/2021/world/covid-vaccinations-tracker.html (Accessed April 14, 2022)
[4] https://www.bbc.com/news/world-56237778
[5]https://www.npr.org/sections/goatsandsoda/2022/03/14/1086474455/the-goal-vaccinate-70-of-the-world-against-covid-scientists-are-proposing-a-rebo
[6]https://www.statnews.com/2021/12/13/we-have-enough-covid-vaccines-for-most-of-world-but-rich-countries-stockpiling-more-than-they-need/
[7] https://www.state.gov/covid-19-recovery/vaccine-deliveries/ (Accessed April 15, 2022)
[8]https://www.nytimes.com/2022/04/04/us/politics/senate-covid-vaccines.html?searchResultPosition=2
[9] https://www.youtube.com/watch?v=B8UEZ9cfgz4v
[10] https://now.tufts.edu/articles/how-viruses-mutate-and-create-new-variants
[11] https://www.sciencedirect.com/science/article/pii/S1201971221008572)
[12] https://covid.cdc.gov/covid-data-tracker/#rates-by-vaccine-status
[13] https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2790204
[14] https://www.cidrap.umn.edu/news-perspective/2021/12/cdc-advisors-recommend-mrna-covid-vaccines-over-jj
[15] https://www.cnbc.com/2021/01/28/why-mrna-vaccines-like-covid-vaccines-are-more-flexible-to-variants.html
[16] https://www.nature.com/articles/s41562-022-01304-y
[17] https://newrepublic.com/article/162527/long-strange-trips-grubby-history-vaccines-became-intellectual-property)
[18] https://www.politico.eu/article/compromise-reached-on-covid-19-vaccine-intellectual-property-rights-waiver/?link_id=1&can_id=b645707b2a6858d667c1f090744bfb41&source=email-monday-emergency-briefing-on-leaked-vaccine-waiver-pproposal&email_referrer=email_1481793&email_subject=monday-emergency-briefing-on-leaked-vaccine-waiver-proposal)
[19] https://www.mckinsey.com/industries/public-and-social-sector/our-insights/port-to-patient-improving-country-cold-chains-for-covid-19-vaccines)
[20] https://thecolumn.substack.com/p/bidens-new-covid-czar-previously?s=r
[21] Sher AD. A beautiful idea: how COVAX has fallen short. The Lancet World Report. 2021;397:2322-2325
[22]https://www.precisionvaccinations.com/vaccines/corbevax-covid-19-vaccine
[23] texastribune.org/2022/02/10/corbevax-texas-coronavirus-vaccine
[24]https://allianceforscience.cornell.edu/blog/2022/01/corbevax-a-new-patent-free-covid-19-vaccine-could-be-a-pandemic-game-changer-globally