The Weather
This week we’ll see the last of the data from the pre-holiday season being reported on. In the next few weeks, we will likely start to see the beginnings of how COVID trends will shake out over the winter season. Remember to wear high quality masks such as N95s, KN95s and KF94s in indoor public spaces and outdoors at protests and in crowds, and to carry extras for yourself and others this holiday season and always.
Wins
In response to your public comments, the Centers for Medicare and Medicaid Services (CMS) COVID Hospitalization reporting requirements started on November 1. Public-facing data is now available via the NHSN Hospital Respiratory Data (HRD) Dashboard.
This past Thursday, Native Americans and others gathered for the 54th annual National Day of Mourning in Plymouth, MA. Masks were required (and worn by most) as they have been since the pandemic’s start. Epidemics were a key weapon in genocides across North America, and disease continues to be a weapon of war and colonization. Our struggles are interconnected. We salute Indigenous struggles for sovereignty here and across the world.
Many protests for an end to the siege on Gaza and Lebanon occurred across the nation during the most recent holiday and black friday. In New York City, 21 protesters successfully interrupted and delayed the annual Macy’s Thanksgiving Day Parade for 5 minutes with a banner that read “Land Back! Don’t Celebrate Genocide! Free Palestine! Arms Embargo Now!” before being brutally detained by the NYPD. All but 3 of these protestors wore masks despite the pouring rain. We commend them for setting the bar and protecting their health and right to privacy even outdoors, and even during a high-stress, high arrest-risk-level action.
For more information on why it’s important to wear masks at protests and on the history of correlation between those most vulnerable to disability and targets of police violence as a whole, visit our toolkit on COVID Safety for Protests.
Wastewater
Wastewater reporting on the period from November 10–16 is continually updated as data from each state that was not ready at the time of the initial publish continues to roll in. In this week’s CDC national wastewater map, we can see that in the most recent data from November 21st, three more states have been moved into the “Moderate” to “Very High” categories and that several states within those categories have been updated to depict higher levels of virus than were available to us at the time of the first reporting of the wastewater levels for this time period two weeks ago. As we sit in this brief period of CDC holiday break between in updates, waiting for the initial or first-impressions data from the last two weeks to be posted, we remind you to always also look at data for your specific region, either through the CDC portal or on local portals, such as this one for New York State, if they are available in your region. You can also check sites like Wastewater Scan which are updated with a different frequency. Additionally, always check back at wastewater data in the weeks after its first posting for the full picture, and remember to take the first data that’s posted as an outline or first impression.
In this November 21st update, Arizona, Mississippi, Ohio, Oklahoma and South Dakota are reporting limited coverage. No data is available for Guam, North Dakota, and the US Virgin Islands.
And as always, remember that the levels of COVID in the wastewater that have been matched to the map categories of “Very High”, “High”, “Moderate”, “Low” and “Minimal” have not been tested to reflect one’s risk of getting sick in each region in any given time, these naming conventions are completely independent of any relationship to community transmission. Wastewater data is an important tool that is best used to tell if levels in your area are increasing or decreasing, which is good for charting the course of the pandemic as a whole. But it can not predict your likelihood of getting sick at any given time.
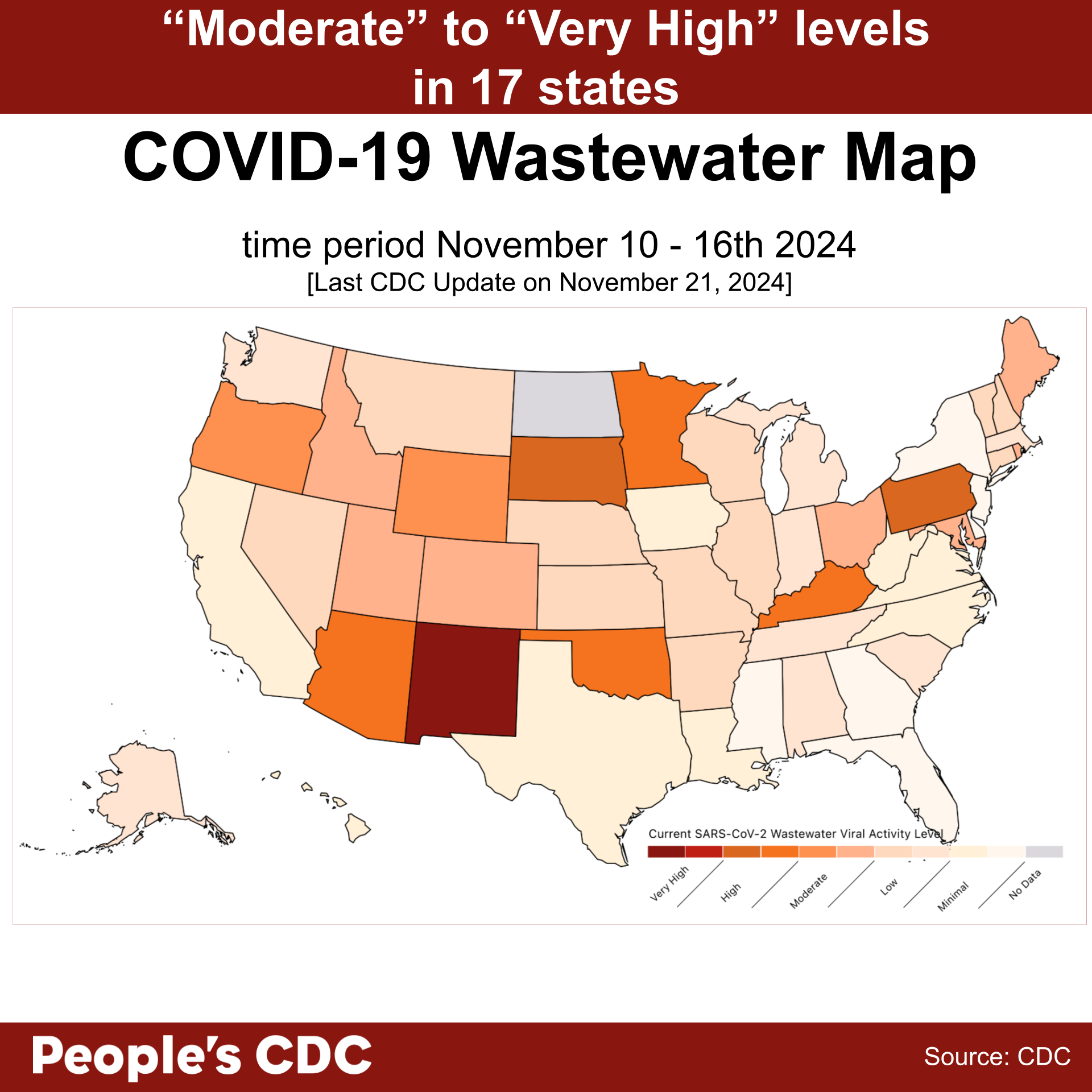
Graphic source: CDC
The Wastewater COVID-19 National and Regional Trends dashboard most recent update (on November 21st) of data reported from the week ending in November 16th shows an average of “low” levels with a slight increase in the midwest, northeast, and west regions from 2.13, 1.12, 2.14, to 2.27, 1.24, 2.17, respectively. If we look at data from last year and the years before as a prediction, we are likely in the eye of the storm period after the summer surge has settled and just at the starting point of the winter surge beginning to form. But the wastewater data for the period that we are living now will not come out for another couple of weeks, as wastewater data typically tells us the story of where viral-concentration levels were 2 prior to the present moment. Remember to use layers of protection to flatten the curve and break chains of transmission this winter surge season.
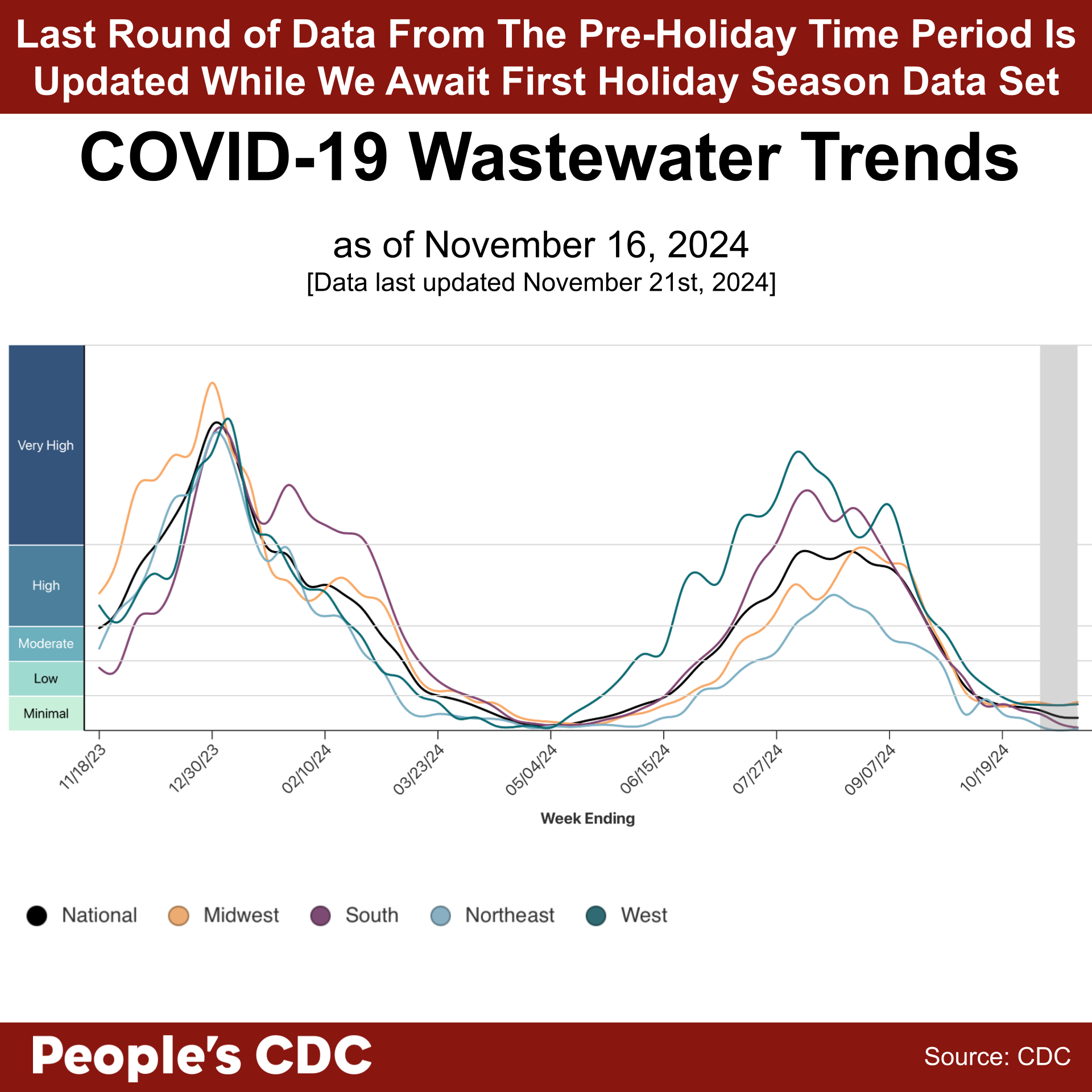
Graphic source: CDC
Variants
According to the CDC’s variant tracking dashboard, recombinant variant XEC (a combination of two JN.1-derived variants: KS.1.1 and KP.3.3) is increasing and is projected to rise to 38%, almost on equal footing with KP.3.1.1 at 44%, by November 23rd. All of the currently displayed variants are derived from JN.1-based lineages, meaning that our current vaccines (Pfizer, Moderna, and Novavax) based on JN.1 itself (Novavax) or the more recently emerged KP.2 sublineage of JN.1 (Pfizer and Moderna) are anticipated to be well-matched and effective.
It is not too late to get an updated vaccination if you haven’t already. Visit the national vaccine finder to find options in your area. Contact your local health department to ask about free and low-cost COVID and flu vaccine events in your area.
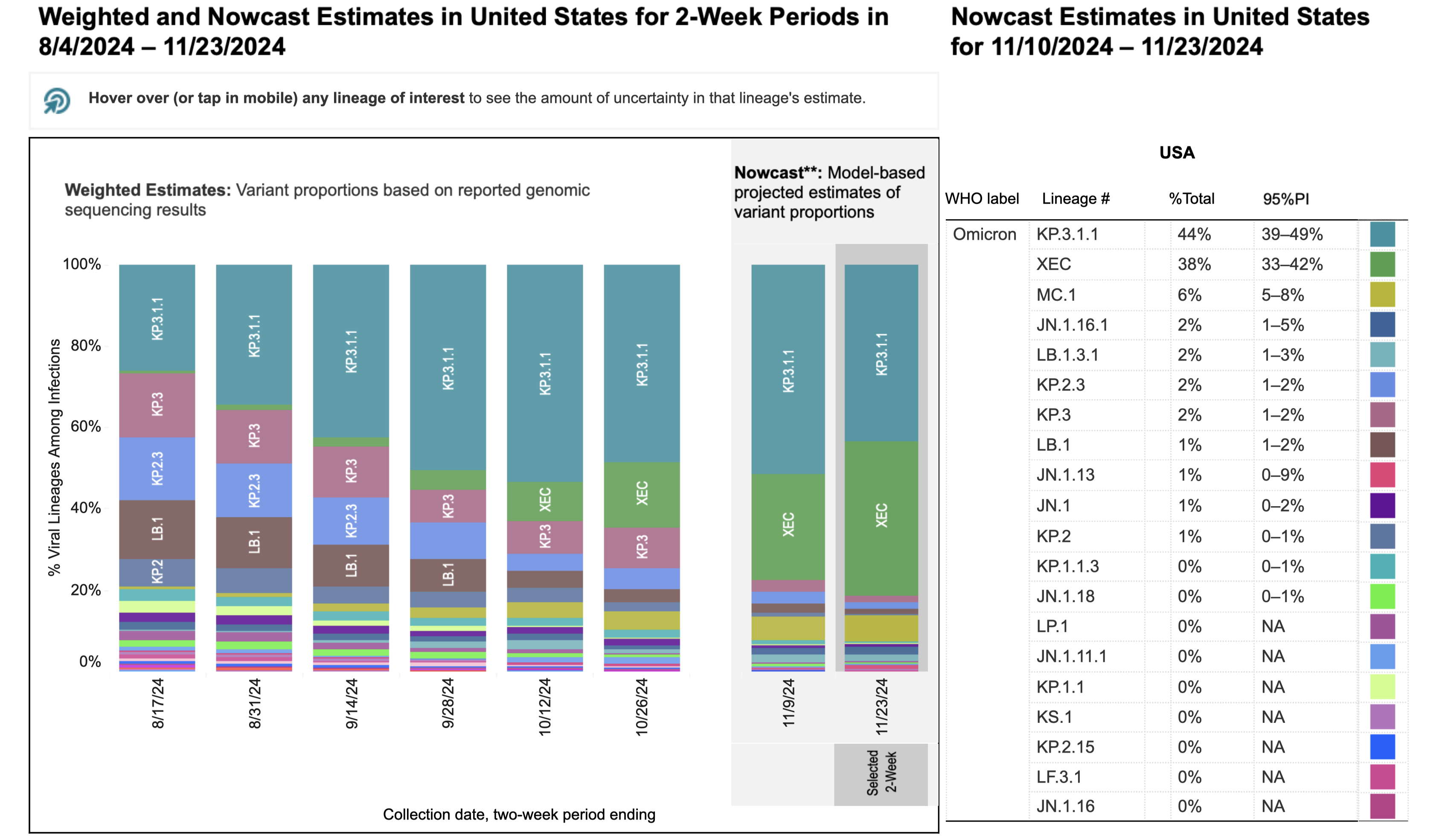
Graphic source: CDC Variant Tracker
Positive Effects of Masking and Testing in Healthcare Settings
A new study titled “Testing and Masking Policies and Hospital-Onset Respiratory Viral Infections” used data from November 6, 2020–March 21, 2024 to compare positive hospital viral rates of influenza, RSV, and COVID for patients who developed infections as a cause of their stay in the hospital, and those who were infected prior to hospitalization but did not develop symptoms until their period of hospitalization, during the pre-Omicron period, the Omicron period with mandatory testing and masking, Omicron without mandatory testing and masking, and Omicron after restarting masking for healthcare workers alone. Results showed that the end of mandatory masking and testing was “associated with a 25% increase in hospital-onset respiratory viral infections compared with the preceding Omicron-dominant period…and resumption of masking among staff [only] was associated with at 33% decrease in hospital-onset respiratory viral infections.”
In the same study, in a randomly selected pool of 100 patients who tested positive for COVID in the hospital after mandatory testing during the admissions process was terminated, 89 of 100 had new symptoms, only 27 of 100 had a known COVID exposure, and 8 of 100 died in-hospital.
Hospitals, clinics, and dentists offices are where we go when our health is at its weakest. We must advocate for these facilities to use all methods of infection control available to them. More info on how to support these efforts below in our Take Action section.
Take Action
Sunday, December 1st is World AIDS Day, with events across the nation and around the globe taking place throughout the week. Find an event in your area and take this time to learn from those who have advocated for care in previous generations and who continue to advocate for treatment in the face of stigma and criminalization as new pandemics arise and unfold concurrently. Get tested, know your status and stay up to date on options for prevention such as condoms and PrEP and PEP for those sexually active of all genders, and all sexualities, at all ages, and also for those who use injection drugs, because just like COVID, HIV transmission is not over—and you may be at risk without knowing it. And similar to the fight for recognition, clinical studies, and robust access to long term care for those diagnosed with Long COVID, a first generation of long-term survivors of AIDS and HIV are now reaching retirement age. We must continue to fight for studies for new, innovative, and affordable treatments for long-term survivors and ultimately, for a cure.
Support masking in healthcare by writing to your local, state, and federal elected officials.
Call your local and state elected officials and ask if they have heard of any plans to introduce mask bans in your area, and regardless of their answer, register your dissent. Invite one friend to do the same. Visit our website for more background on the rising threat of mask bans.
We continue to rely on COVID wastewater testing to get a better understanding of COVID spread nationally and within our communities. Let your federal elected officials know that COVID wastewater monitoring must expand and continue. If you live in an area with no data or limited data, consider writing to state and local officials to ask them to fund wastewater surveillance in your area.
Volunteer and find support with a Mask Bloc or other COVID Action group in your area. Taking action together we can create larger and larger waves of change.
Notes: 1) The numbers in this report were current as of 11/29/2024. 2) Check out the links throughout & see our website for more at https://peoplescdc.org. 3) Subscribe to our newsletter: People’s CDC | Substack.